A clinical trial is a planned experimental study on humans designed to evaluate new interventions (e.g. type or dose of drug, or surgical procedure) compared to a comparative treatment.
14.2 Phases of Clinical Trials
There are several different stages of clinical trials:
code
phases <-tibble(Phase =c("Phase I", "Phase II", "Phase III", "Phase IV"),Purpose =c("Establish dosage, side effects and delivery mechanisms","Investigate treatment effects and safety in small studies","Full evaluation of new treatment compared to comparator","Observe how treatment works in non-trial setting" ),`Sample Size`=c("Small (20-80)", "Moderate (100-300)", "Large (1000+)", "Very large"),Focus =c("Safety, dose-finding","Efficacy, optimal dosing","Effectiveness vs standard care","Long-term effects, rare side effects" ))phases |>kable() |>kable_styling(bootstrap_options =c("striped", "hover"))
Table 14.1: Phases of clinical trials
Phase
Purpose
Sample Size
Focus
Phase I
Establish dosage, side effects and delivery mechanisms
Small (20-80)
Safety, dose-finding
Phase II
Investigate treatment effects and safety in small studies
Moderate (100-300)
Efficacy, optimal dosing
Phase III
Full evaluation of new treatment compared to comparator
Large (1000+)
Effectiveness vs standard care
Phase IV
Observe how treatment works in non-trial setting
Very large
Long-term effects, rare side effects
Phase I & II trials are pre-clinical or small studies which investigate treatment effects and safety. They establish dosage, side effects and delivery mechanisms.
A Phase III trial is a full evaluation of the new treatment compared to a comparative treatment.
After a treatment has been approved and licensed for general use, Phase IV trials observe how the treatment works in a non-trial setting, identify long-term effects and rare side effects.
14.3 Control Groups
Phase III trials have at least one treatment group and comparator group (the control group).
If the condition under investigation has a standard treatment, then this is the treatment that the control group may receive
If standard care does not exist, then the control might be given a placebo (a treatment which does not consist of an active component) or no treatment if considered ethical
The purpose of the control group is to quantify the effect of the treatment by comparing the outcome of interest in the control group to the outcome in the treatment group.
14.4 Treatment Allocation (Randomisation)
Patients are usually randomised to treatment groups. This is to avoid systematic bias, and ensure that each patient has an equal chance of being allocated to each treatment.
Methods of Randomisation
code
randomisation <-tibble(Method =c("Simple randomisation", "Block randomisation", "Stratified randomisation", "Cluster randomisation"),Description =c("Each patient randomly allocated to treatment (like flipping a coin)","After every x patients, number on each treatment is equal","Block randomisation within important prognostic strata (e.g. age, stage)","Groups/clusters of individuals randomised rather than individuals" ),Advantage =c("Simple to implement","Ensures balanced numbers in each arm","Balances important prognostic factors","Practical when individual randomisation not possible" ))randomisation |>kable() |>kable_styling(bootstrap_options =c("striped", "hover"))
Table 14.2: Methods of randomisation in clinical trials
Method
Description
Advantage
Simple randomisation
Each patient randomly allocated to treatment (like flipping a coin)
Simple to implement
Block randomisation
After every x patients, number on each treatment is equal
Ensures balanced numbers in each arm
Stratified randomisation
Block randomisation within important prognostic strata (e.g. age, stage)
Balances important prognostic factors
Cluster randomisation
Groups/clusters of individuals randomised rather than individuals
Practical when individual randomisation not possible
14.5 Allocation Concealment (Blinding)
Randomisation is not sufficient to ensure that a trial is unbiased. If outcome assessment is subjective or open to interpretation, systematic bias can be introduced by knowledge of the treatment received.
Masking or blinding means that people are unaware of the treatment that someone received.
Levels of Blinding
Level
Description
Single blind
The patient does not know which treatment they have been allocated
Double blind
Neither patient nor doctor/evaluator knows which treatment has been allocated
Triple blind
Neither the patient, nor the doctor, nor those reviewing the interim results know which treatment the patient has been allocated
14.6 Designs for Randomised Trials
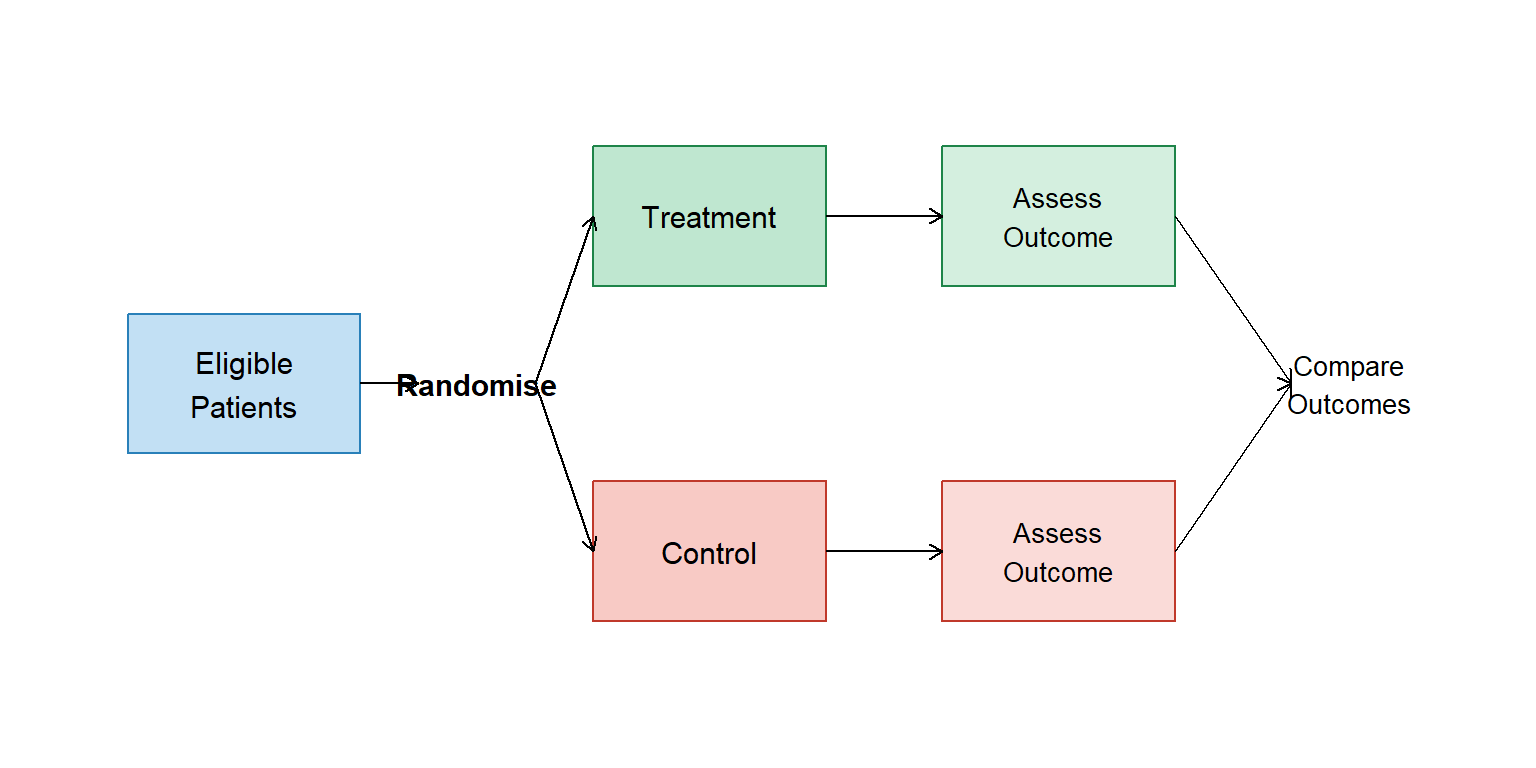
Parallel Groups
The simplest form of randomised trial is a parallel group trial. Eligible patients are randomised to two or more groups, treated according to the assigned group, and assessed for their response to treatment.
code
# Simple diagramggplot() +# Population boxannotate("rect", xmin =0, xmax =2, ymin =2, ymax =3, fill ="#3498db", alpha =0.3, colour ="#2980b9") +annotate("text", x =1, y =2.5, label ="Eligible\nPatients", size =4) +# Randomisationannotate("text", x =3, y =2.5, label ="Randomise", size =4, fontface ="bold") +# Treatment armannotate("rect", xmin =4, xmax =6, ymin =3.2, ymax =4.2, fill ="#27ae60", alpha =0.3, colour ="#1e8449") +annotate("text", x =5, y =3.7, label ="Treatment", size =4) +# Control armannotate("rect", xmin =4, xmax =6, ymin =0.8, ymax =1.8, fill ="#e74c3c", alpha =0.3, colour ="#c0392b") +annotate("text", x =5, y =1.3, label ="Control", size =4) +# Outcome boxesannotate("rect", xmin =7, xmax =9, ymin =3.2, ymax =4.2, fill ="#27ae60", alpha =0.2, colour ="#1e8449") +annotate("text", x =8, y =3.7, label ="Assess\nOutcome", size =3.5) +annotate("rect", xmin =7, xmax =9, ymin =0.8, ymax =1.8, fill ="#e74c3c", alpha =0.2, colour ="#c0392b") +annotate("text", x =8, y =1.3, label ="Assess\nOutcome", size =3.5) +# Arrowsannotate("segment", x =2, xend =2.5, y =2.5, yend =2.5,arrow =arrow(length =unit(0.2, "cm"))) +annotate("segment", x =3.5, xend =4, y =2.5, yend =3.7,arrow =arrow(length =unit(0.2, "cm"))) +annotate("segment", x =3.5, xend =4, y =2.5, yend =1.3,arrow =arrow(length =unit(0.2, "cm"))) +annotate("segment", x =6, xend =7, y =3.7, yend =3.7,arrow =arrow(length =unit(0.2, "cm"))) +annotate("segment", x =6, xend =7, y =1.3, yend =1.3,arrow =arrow(length =unit(0.2, "cm"))) +# Compareannotate("segment", x =9, xend =10, y =3.7, yend =2.5,arrow =arrow(length =unit(0.2, "cm"))) +annotate("segment", x =9, xend =10, y =1.3, yend =2.5,arrow =arrow(length =unit(0.2, "cm"))) +annotate("text", x =10.5, y =2.5, label ="Compare\nOutcomes", size =3.5) +theme_void() +coord_cartesian(xlim =c(-0.5, 11.5), ylim =c(0, 5))
Figure 14.1: Schematic of a parallel group trial design
Factorial Designs
In a factorial trial, two (or more) intervention comparisons are carried out simultaneously.
For example, in a trial for surgical patients with colorectal cancer, those who participate might be randomised to:
Receive peri-operative radiotherapy or not, AND
Receive local regional chemotherapy or not
Most factorial trials have two ‘factors’, each of which has two levels. This is called a 2×2 factorial trial, and gives 4 combinations of treatment:
Table 14.3: Treatment combinations in a 2×2 factorial trial
No radiotherapy
Radiotherapy
No chemotherapy
Neither treatment
Radiotherapy alone
Chemotherapy
Chemotherapy alone
Both treatments
Potential problems:
Treatment effects may not be additive (interaction)
Must be practical to combine treatments
Toxicity of combined treatment must be acceptable
Cross-over Trials
In a cross-over trial, every patient receives all treatments under investigation, but the order in which they receive them is randomised.
In the case of a two-treatment cross-over trial, eligible patients are randomised to receive either:
Treatment A followed by Treatment B, OR
Treatment B followed by Treatment A
Benefits:
Each patient acts as their own control
Effectively leads to a smaller sample size - halving the number of patients when compared to a conventional parallel design
Potential problems:
Drop-out after the first treatment (which may be related to treatment)
Carry-over of treatment effects from the first period which is not eliminated by a wash-out period
Treatment-period interaction – in which the effect of a treatment is substantially different in the two periods
14.7 Analysis of Clinical Trial Data
Intention-to-Treat Analysis
Randomised controlled trials often suffer from noncompliance, drop-outs and missing outcomes.
An analysis based only on those patients who completed the study without protocol violations (per-protocol population) can introduce bias and lead to an overestimation of effectiveness. This is because the reason why patients do not comply or drop out may be related to the treatment they received.
One potential solution is called intention-to-treat (ITT) analysis. ITT analysis includes every subject who was randomised according to the randomised treatment assignment. It ignores noncompliance, protocol deviations, withdrawal, and anything that happens after randomisation.
Key Point
In ITT analysis, the estimate of treatment effect will generally be more conservative than that found with a per-protocol analysis.
Number Needed to Treat (NNT)
The NNT is the number of patients that need to be treated for one patient to benefit from a treatment compared to a control treatment.
The absolute risk reduction is the risk in control group minus the risk in treatment group.
NNT
Interpretation
1
Everyone improves with treatment and no one improves with control
Higher values
Less effective treatment (more patients need to be treated for one to benefit)
14.8 Outcome Measures in Oncology Trials
code
endpoints <-tibble(Endpoint =c("Overall survival (OS)", "Progression-free survival (PFS)", "Disease-free survival (DFS)", "Objective response rate (ORR)","Tumour regression", "Quality of life", "Toxicity"),Description =c("Time from randomisation to death from any cause","Time from randomisation to progression or death","Time from randomisation to recurrence or death (after curative treatment)","Proportion with complete or partial response","Reduction in tumour size","Patient-reported outcomes on wellbeing","Adverse events and side effects" ))endpoints |>kable() |>kable_styling(bootstrap_options =c("striped", "hover"))
Table 14.4: Common outcome measures in oncology clinical trials
Endpoint
Description
Overall survival (OS)
Time from randomisation to death from any cause
Progression-free survival (PFS)
Time from randomisation to progression or death
Disease-free survival (DFS)
Time from randomisation to recurrence or death (after curative treatment)
Objective response rate (ORR)
Proportion with complete or partial response
Tumour regression
Reduction in tumour size
Quality of life
Patient-reported outcomes on wellbeing
Toxicity
Adverse events and side effects
14.9 CONSORT Statement
CONSORT stands for Consolidated Standards of Reporting Trials. The CONSORT statement is a set of recommendations for the standardised reporting of randomised trials. It is used to aid transparency, critical appraisal and interpretation.
The CONSORT statement contains:
A 25-item checklist ensuring information on trial design, participants, treatment allocation, analysis, interpretation and limitations is included
A flow diagram displaying for each group:
Numbers of participants randomly assigned
Numbers who received intended treatment
Numbers analysed for the primary outcome
Losses and exclusions after randomisation
14.10 Summary
Concept
Description
Clinical trial
Planned experimental study to evaluate interventions
Phase I/II
Safety and dose-finding studies
Phase III
Full efficacy evaluation vs comparator
Phase IV
Post-marketing surveillance
Randomisation
Random allocation to ensure equal chance of treatment